Handbook of Cannabis edited by Roger G. Pertwee was published in august 2014, containg 40 chapters. This summary of chapter 17: Self-Medication with Cannabis is written by authors Arno Hazekamp & George Pappas & are both connected to Bedrocan, the Dutch Medical Cannabis Grower Company for the Dutch Government’s Health department.
Intro
Since the United Nations adopted the Single Convention on Narcotic Drugs in 1961 cannabis & its products have been defined as ‘narcotics with high potential for abuse & no accepted medicinal value‘. This strict legal classification has effectively delayed their progression into modern medicine, by not only keeping cannabis & cannabinoids out of the hands of medical users, but also by depriving researchers of the materials needed for scientific investigation. Despite its illegality large numbers of patients have continued to push for the right to use cannabis, including the right for selfmedication.
The medical use of cannabis is slowly gaining more acceptance worldwide, specially with quality controlled herbal cannabis programs like the Netherlands since 2003 & Canada since 2001. Many American States have introduced laws as well to permit medical marijuana use & patients grow their own, although almost no official quality control standards have been released so far. In any case it is left to patients themselves how to administer the herb. Self-medication with cannabis is therefore the most common way of using cannabinoids medicinally.
There is still much to learn about the risks of potential contaminations with pesticides, growth-enhancing chemicals, microbes or heavy metals, especially in the absence of quality control with all the differences of cannabis varieties.The synergy of cannabis components & the sociocultural role of cannabis still have to be examined futher. Psysicians are often hesitant to play a role of prescriber, even in the official government countries running medical cannabis programs. It ’s about finding a balance between requirements of medical authorities & policymakers with standardisation, quality control & safety, as well as those of patients & their physicians with choise of variety, administration form of whole plant preparations. Ensuring to advance the scientific understanding of cannabis-use is the key. Cannabis is on the hand too potent to be regulated as an herbal alternative medicine, on the other hand too herbal to be considered as conventional medicine.
Reason
The reason that people choose selfmedication over more conventional therapy are cost issues, distrust in modern medicine, or an interest in ‘green’ medicine & even interest in the underlying cannabis subculture with a wide range of choises on chemical variety among cannabis strains & administration forms. Despite the fact that cannabis & modern medicine have an uneasy relationship with each other, it seems that the medical use of cannabis is here to stay.
Selfmedication can be seen as a positive way to empower patients to take greater control over their care, and to increase healthcare efficiency by reducing doctor visits. Allowance for medicinal use of cannabis simply requires an authorisation signed by a physician to recieve protection from legal penalties. The patients are essentially left to use the cannabis on their own, without dosage instructions or efficacy in disease progression. Evidence based monitoring of the efficacy of cannabis on the indications for which is used & even whetether it is being used for effectively & responsibly is almost entirely lacking. As cannabis is by far the most widely used illicit drug in Western cultures, some people may initially use cannabis recreationally but then discover, consciously or subconsciously an improvement of symptoms of a diagnosed or undiagnosed condition. The potentially fine line between proper self-medicating of a medical condition & using cannabis in situations where it may do more harm than good, a better understanding of the choises, preferences & motivations of patients is a good starting point in our exploration of self-medicating with cannabis.
Effects
There are an estimated 119-224 million frequent users of cannabis worldwide (UN 2012) but it is unclear how many of them could be considered or consider themselves as medicinal users, while a number of 80% of the cannabis use in Isreal is medicinal, has been unofficially reported. Currently most information available on the effects of cannabis use comes from studies on the (ab)use of cannabis as a recreational drug. As a result new medical users & their psysicians are often concerned about the risk of addiction, overdosing & intoxication (feeling ‘high’). With the same focus on cannabis it is important to recognize large differences between medicinal & recreational users in terms of intention, frequency and size of dosing & route of administration. An important reason for patients to keep purchasing materials from illicit markets is the fact that, often by trial & error, they claim to have found particular strains that work optimally for treatment of their specific symptoms.
In the context of self-medicating an obvious question is how the chemical constituents found in various cannabis cultivars reflect differential medicinal properties & what types of cannabis should consequently be made available to patients. Mainly cannabis sativa & cannabis indica are typically classified, although most cultivars are however genetically a blend of both types. It is unclear whether this classification reflects any relevant differences in chemical composition.
To bridge the gap between the vast knowedge on cannabis that exists within the community of recreational users & the information needed by medicinal users & health professionals in the understanding of chemical differences the emergence of the PCA-method of identifying & quantifying all major components (cannabinoids & terpenes synergy Russo 2011) present in various cannabis types, is important for identifying specific components on their efficacy. Thus using a comprehensive chemovar approach may help self-medicating users & their physicians to succesfully switch from a beneficial cannabis variety obtained though illicit markets, to a similar strain that is available though official programs of medicinal cannabis. Exchange of cultivars & analytical data between the various cannabis programs worldwide may greatly facilitate such a transition.
Physicians in a Canadian survey worried that patients who requested medical cannabis actually wanted it for recreational purposes & that medical doctors did not have enough information on the risks and benefits or on the appropriate use of cannabis for medical purposes. The discussion of self-medicting with cannabis primary focused on therapeutic benefits versus pharmacological side effects, while additional factors may be involved.
A meta-analysis on the subjective effects of cannabis found that the most frequently reported effects were: improved mood (i.e feeling good, content), enhanced relaxation, increased insight into self & others, & improved perceptions (Green et al. 2003). This indicates that establishing medical efficacy through clinical means alone overlooks a myriad of psychosocial factors. However, focussing mainly on biomedical & technical approaches, public health agencies have not historically learned to incorporate such ideas & find it difficult to provide a clear answer to this development. Definitions of cannabis as a natural herb remedy as opposed to a synthetic pharmaceutical drug may also influence perceptions in favor of its use (Reinarman et al. 2011).
Cannabis clubs
In a study (Feldman & Mandel 1998) looking at the benefits of membership of ‘cannabis (buyers) clubs’ in the US, the authors concluded that such cannabis clubs were the soundest option – compared to doctors, pharmacists, police and the black market – for providing acces to cannabis as medicine. They argue that the clubs afford the best therapeutic setting, a healing environment that offers an ethos of love, compassion & emotional support in addition to health benefits of cannabis itself. The same message was echoed in a study of Hathaway and Rosier (2007) where interviewed members contrasted their compassion clubs with treatments they received at the hands of doctors, welfare agencies, employers, authorities & government officials. A common theme recorded was that ‘chronic illness stigmatizes & subjects those who suffer to shame & institutionalized abuse.’ So perhaps the greatest strength of medicinal cannabis use is in the holistic approach that cannot be found alongside the treatment with conventional drugs today.
Cost
Because chronically ill patients, as a result of disability and unemployment, are often living on a small budget, the reason for choosing to self-medicate may simply be related to the cost. The cost factor might have had substantial influence on available data of self-medication, as it may be a reason for patients to grow their own cannabis, or to choose poorer-quality products jeopardizing their health. Also some patients might be preferring herbal cannabis simply since they need a very high dose of cannabinoids, which cannot be covered by the available pharmaceutical cannabinoid preparations or are currently not covered by heath insurances, both practically & economically.
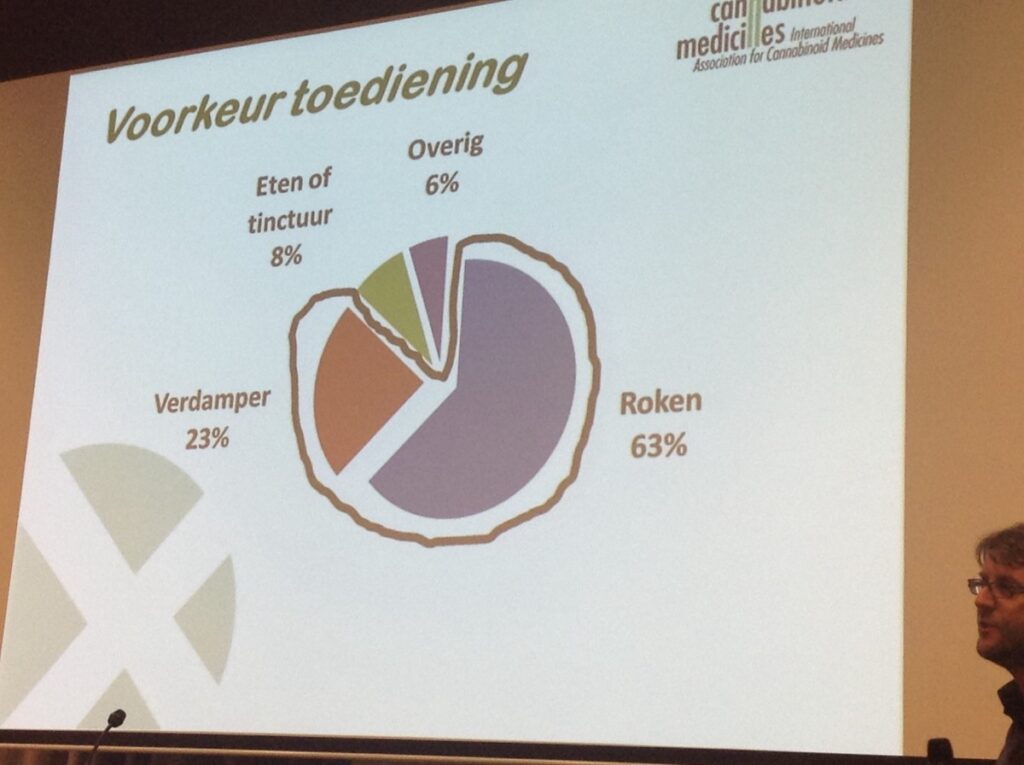
Smoking
Decarboxylation is a conversion process where herbal cannabis essentially convers the acidic cannabinoids into their pharmacologically active counterpart by heating. Overheating as well as exposure to light or air may lead to the formation of degradation products such as CBN/cannabinol & 8 delta-THC, with potential pharmacological properties of their own (Izzo et al. 2009) Fragile components such a the terpenes may get lost by evaporation as a result of long-term storage, or preparation methods that apply heat before consumpion (e.g boiling for tea, evaporating solvents for making extracts). Moreover each administration form comes with its own set of specific metabolites formed upon consumption. As a result of all these factors combined, a different spectrum of compounds is finially entering the bloodstream, & consequently a different type of duration of effects may be observed for each cannabis medicine.
By far smoking is the most commonly used method of consuming cannabis, & is more effective than oral administration. Inhaling is about equal in efficiency to intravenous injection, while considerably more practical. Cannabis smoking is generally appreciated by self-medicating patients allowing accurate self-titration of the desired effects, with some kind of psychoactivity as well. Although use of tobacco should obviously not be encouraged, it may be relevant to futher study wheter the addiction of tobacco to cannabis sigarettes is merely a matter of taste or habit, or has an actual therapeutic function in combination with cannabis. At least one study has suggested that the presence of tobacco releases relatively more THC from cannabis when smoked (van der Kooy et al. 2009). Shortcomings of smoked cannabis i.e inhaling toxic compounds during cannabis smoking have been widely viewed as a major obstacle for approval of herbal medicine by public health authorities.
Vaporizing can be considered an efficient way of cannabinoid administration with a bioavailability comparable to smoking, below the point of combustion where pyrolytic toxic compounds can be released (typically 180-210 degrees celcius) with the whole range of terpenes present in herbal cannabis efficiently inhaled, maximizing therapeutic potential.
Self-medication with cannabis seems to be prominent & rising popularity. As officially and federally regulated medicinal cannabis programs continue to increase in prevalence & size, those who have been pushed into self-medication linked with the illicit market may get the opportunity to bring their medicinal use into the scope of a regular patient-physician relationship. In the ideal setting, physicians should have the information at hand to offer the same care with cannabis as they do with other pharmaceutical preparations. Self-medicaton with cannabis may then become stricktly a matter of choice, rather than necessity.
Amsterdam, november 2014 – drs. Hester Kooistra (University of Humanistic studies) for the Dutch Legalize Foundation.
newsflash
Self-medication with cannabis
29
nov
nov
Summary: Self-medication with cannabis from Hazekamp & Pappas (Handbook of Cannabis) is about the right & acceptance to use cannabis as self medication. Patients grow their own or connect to a cannabis club to obtain their herbal medicine for treatment.